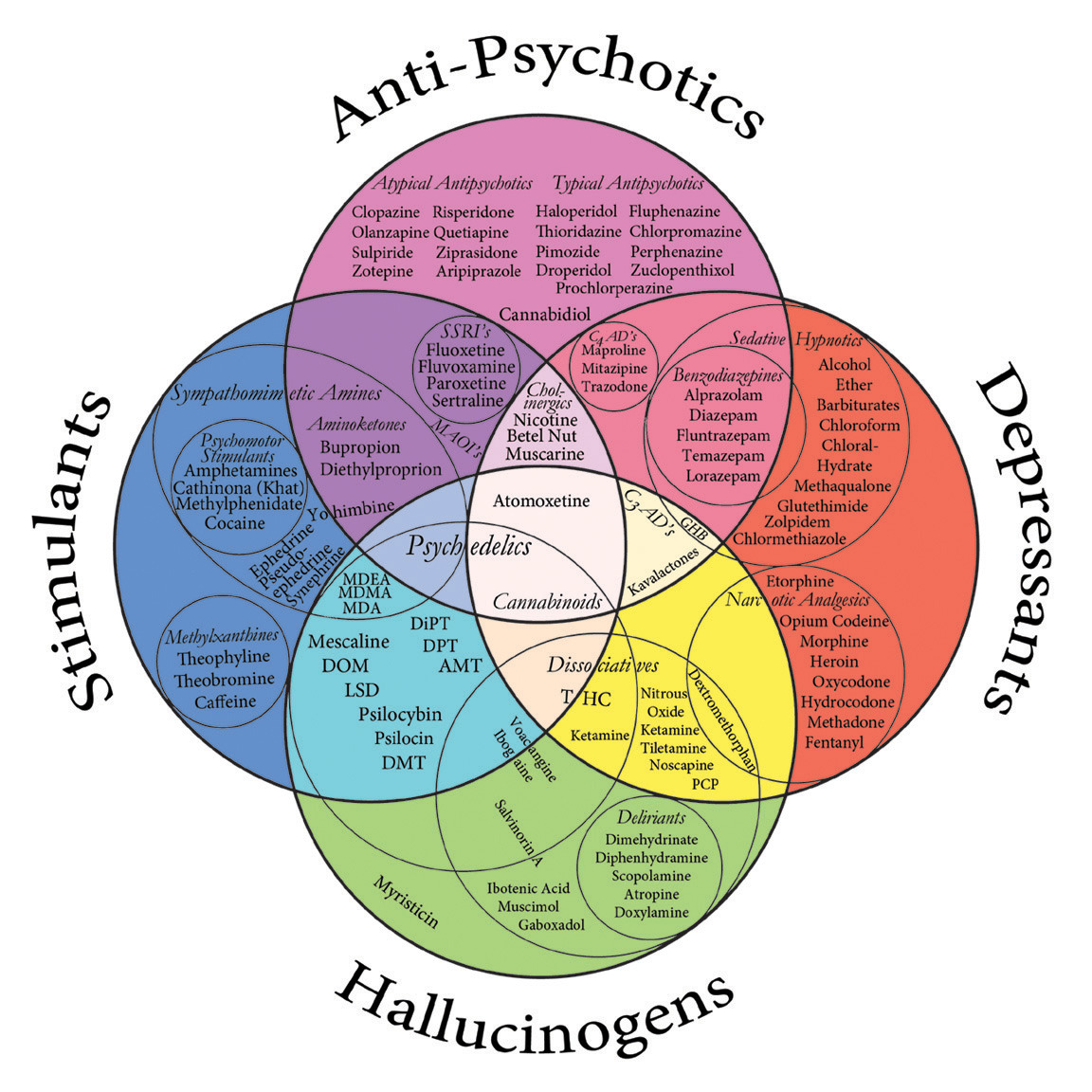
Venn diagram of psychoactive drugs [click for larger image]
NOTE: This post is part of a Nature Blog Focus on hallucinogenic drugs in medicine and mental health, inspired by a recent Nature Reviews Neuroscience paper, The neurobiology of psychedelic drugs: implications for the treatment of mood disorders, by Franz Vollenweider & Michael Kometer. This article will be freely available, with registration, until September 23. For more information on this Blog Focus, see the Table of Contents.
The secret history of psychedelic psychiatry is discussed over at Neurophilosophy. Neuroskeptic covers Serotonin, Psychedelics and Depression while Mind Hacks provides a personal look at yagé in Visions of a psychedelic future.
Veterinary Anesthetic, Club Drug, or Antidepressant?
Club drug "Special K" (aka ketamine) is stepping out of the laser light into the broad daylight of mainstream psychiatry with the publication of a new review article by Vollenweider and Kometer (2010). Long used to anesthetize animals (and children), ketamine was classified as a "dissociative anesthetic" by Domino et al. (1965) for its combined effects of sedation/analgesia and hallucinations. Domino (2010) recently revisited his classic paper, which reported on a study in 20 volunteers incarcerated at the Jackson Prison in Michigan:
The first human was given ketamine in an intravenous subanesthetic dose on August 3, 1964. Guenter [Corssen, M.D.] and I gradually increased the dose from no effect, to conscious but “spaced out,” and finally to enough for general anesthesia. Our findings were remarkable! The overall incidence of side effects was about one out of three volunteers. Frank emergence delirium was minimal. Most of our subjects described strange experiences like a feeling of floating in outer space and having no feeling in their arms or legs.The ego death of the "K hole" can be a terrifying experience for some ("I ceased to exist") or transformative for others ("I witnessed myself as a part of the universal collective of strange energy")1. In their Nature Reviews Neuroscience opinion piece, Vollenweider and Kometer considered ketamine a psychedelic, along with the traditional hallucinogens such as LSD, psilocybin, and mescaline. They noted that both classes of drugs may have psychotherapeutic effects through actions on the excitatory glutamate neurotransmitter system.
Ketamine is an antagonist of the glutamate NMDA receptor and is thought to work by blocking NMDA receptors on inhibitory GABA-containing interneurons, ultimately promoting glutamate release. In a scientific tour de force, Li and colleagues (2010) demonstrated that the mTOR (mammalian target of rapamycin) protein kinase pathway is rapidly activated by ketamine. This sets off a cascade of events including the formation of new synapses on dendritic spines. Using a combination of cellular, molecular, electrophysiological, behavioral, and phamacological techniques, ketamine was shown to exhibit antidepressant properties in animal models of depression and anxiety, perhaps via rapid induction of synaptic plasticity in the medial prefrontal cortex (PFC). Regions of the medial PFC in humans, particularly the ventral anterior cingulate cortex, have been implicated in the pathophysiology of major depression.
Human clinical trials of ketamine as a rapidly acting antidepressant aren't especially new. A randomized, double-blind study in 2000 involved administration of saline or a single subanesthetic dose of ketamine (0.5 mg/kg intraveneously) to nine depressed patients, seven of whom completed the trial (Berman et al., 2000). Within 72 hrs, amelioration of depressive symptoms was observed. Half of the treated patients showed a 50% or greater improvement in depression scores. However, these therapeutic effects weren't very long-lasting, returning to baseline levels in 1-2 weeks. In a larger study, 18 patients with major depression participated in a similar double-blind cross-over design where they received the 0.5 mg/kg dose of ketamine and placebo one week apart (Zarate et al., 2006). The patients were rated at baseline and at 40, 80, 110, and 230 minutes and 1, 2, 3, and 7 days post-infusion on a number of clinical scales, including the Hamilton Depression Rating Scale (HDRS), the Brief Psychiatric Rating Scale (BPRS) positive symptoms subscale, and the Young Mania Rating Scale (YMRS).
The primary outcome measure was change in HDRS score, shown in Figure 2 below (top graph). Significant improvements began at the 110 min time point. Scores declined further from 1-3 days and remained below placebo levels for 7 days. However, unusual experiences were noted at 40 min, with substantial increases in scores for psychosis-like and mania-like symptoms. Other adverse events associated with ketamine included...
...perceptual disturbances, confusion, elevations in blood pressure, euphoria, dizziness, and increased libido. ... The majority of these adverse effects ceased within 80 minutes after the infusion. In no case did euphoria [YMRS] or derealization/depersonalization [BPRS] persist beyond 110 minutes (Figure 2, middle and bottom graphs).

Figure 2 (Zarate et al., 2006). Change in the 21-item HDRS, BPRS positive symptoms subscale, and YMRS scores over 1 week (n=18). Values are expressed as generalized least squares means and standard errors for the completer analysis. * indicates P<.05; †, P<.01; ‡, P<.001.
So here we have several research groups that say yay! to ketamine as an antidepressant. Are there any naysayers?
Although the immediate onset of symptom amelioration gives ketamine a substantial advantage over traditional antidepressants (which take 4-6 weeks to work), there are definite limitations (Tsai, 2007). Drawbacks include the possibility of ketamine-induced psychosis (Javitt, 2010), limited duration of effectiveness (aan het Rot et al., 2010), potential long-term deleterious effects such as white matter abnormalities (Liao et al., 2010), and an inability to truly blind the ketamine condition due to obvious dissociative effects in many participants.
At present, what are the most promising uses for ketamine as a fast-acting antidepressant? Given the disadvantages discussed above, short-term use for immediate relief of life-threatening or end-of-life depressive symptoms seem to be the best indications.
Suicidal Ideation
Acute ketamine treatment in suicidal patients presenting at the ER has the potential to provide immediate changes in the risk that a patient will harm herself when released, when accompanied by proper followup and appropriate long-term treatment. An open label study in 33 patients with refractory depression involved infusion of 0.5 mg/kg ketamine over a period of 40 min (DiazGranados et al., 2010). Those with high scores on the Scale for Suicide Ideation showed significant improvements at 40 min that were maintained for the 230 min duration of the study. Obviously, one would like to follow actively suicidal patients for a longer period of time than 4 hrs, and future clinical trials should take this into account.
Palliative Care
Watching a terminally ill loved one suffer from unbearably excruciating pain is one of the most emotionally wrenching experiences you'll ever have. Anything, and I mean anything2, that will relieve this sort of suffering should be freely administered without reservation or stigma. As discussed in The secret history of psychedelic psychiatry, psilocybin has been shown to alleviate anxiety and pain in cancer patients. Reports of psychedelic psychotherapy in the 60s and 70s suggested that many patients overcame their fear of death through LSD-facilitated sessions. More recently, an open label study in two hospice patients, each with a prognosis of only weeks or months to live, showed beneficial effects of ketamine in the treatment of anxiety and depression (Irwin & Iglewicz, 2010). A single oral dose produced rapid improvement of symptoms and improved end of life quality. To disentangle the pain relieving and antidepressant effects of ketamine, the authors emphasized the importance of conducting clinical trials for this particular indication.
Better Drugs for a Brighter Tomorrow
Newer NMDA antagonist drugs with fewer dissociative side effects (e.g., more selective antagonists such as NR2B receptor blocker EVT 101) are undergoing testing and development. Personalized medicine and pharmacogenomics may ultimately shift psychedelic experiences out of the realm of hippies and into the doctor's arsenal.
ADDENDUM: Moheb Costandi summarizes all four posts in this article for The Guardian, and there's more coverage at The Great Beyond, 3 Quarks Daily, The Atlantic, and Boing Boing.
Footnotes
1 Personal communication and Erowid Experience Vault.
2 Heroin.
References
aan het Rot M, Collins KA, Murrough JW, Perez AM, Reich DL, Charney DS, Mathew SJ. (2010). Safety and efficacy of repeated-dose intravenous ketamine for treatment-resistant depression. Biol Psychiatry 67:139-45.
Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH. (2000). Antidepressant effects of ketamine in depressed patients. Biol Psychiatry 47:351-4.
DiazGranados N, Ibrahim LA, Brutsche NE, Ameli R, Henter ID, Luckenbaugh DA, Machado-Vieira R, Zarate CA Jr. (2010). Rapid resolution of suicidal ideation after a single infusion of an N-methyl-D-aspartate antagonist in patients with treatment-resistant major depressive disorder. J Clin Psychiatry. Jul 13. [Epub ahead of print]Domino EF. (2010). Taming the ketamine tiger. Anesthesiology 113:678-84.
Domino EF, Chodoff P, Corssen G. (1965). Pharmacologic Effects of CI-581, a New Dissociative Anesthetic, in Man. Clin Pharmacol Ther. 6:279-91.
Irwin SA, Iglewicz A. (2010). Oral ketamine for the rapid treatment of depression and anxiety in patients receiving hospice care. J Palliat Med. 13:903-8.
Javitt DC. (2010). Glutamatergic theories of schizophrenia. Isr J Psychiatry Relat Sci. 47:4-16.
Li N, Lee B, Liu RJ, Banasr M, Dwyer JM, Iwata M, Li XY, Aghajanian G, Duman RS. (2010). mTOR-dependent synapse formation underlies the rapid antidepressant effects of NMDA antagonists. Science 329(5994):959-64.
Liao Y, Tang J, Ma M, Wu Z, Yang M, Wang X, Liu T, Chen X, Fletcher PC, Hao W. (2010). Frontal white matter abnormalities following chronic ketamine use: a diffusion tensor imaging study. Brain 133:2115-22.
Tsai GE. (2007). Searching for rational anti N-methyl-D-aspartate treatment for depression. Arch Gen Psychiatry 64:1099-100; author reply 1100-1.
Vollenweider, F., & Kometer, M. (2010). The neurobiology of psychedelic drugs: implications for the treatment of mood disorders Nature Reviews Neuroscience, 11 (9), 642-651 DOI: 10.1038/nrn2884
Zarate CA Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, Charney DS, Manji HK. (2006). A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry 63:856-64.
Dedication:
For my father.




{kind=link}