
Resurrection, Raffaellino del Garbo (1510)
In the world outside of Christianity, horror, and science fiction, the dead cannot be brought back to life. Or can they? A feature in the The Observer from earlier this year profiled Dr. Sam Parnia, critical care physician and author of Erasing Death: The Science That Is Rewriting the Boundaries Between Life and Death (called The Lazarus Effect in the UK). The article begins in a dramatic fashion:
Sam Parnia – the man who could bring you back from the dead
Sam Parnia MD has a highly sought after medical speciality: resurrection. His patients can be dead for several hours before they are restored to their former selves, with decades of life ahead of them.
That's a pretty outrageous claim! Clinically dead for several hours? No brain activity the entire time? Even if anyone could emerge alive and conscious from such a state (unless it's a state of suspended animation, perhaps), they'd have severe brain damage (as we'll see below). There'd be no way they could have encoded their near-death experiences (NDEs), much less remembered any light at the end of a tunnel or a soothing presence drawing them home.
There may be a semantic problem here: the definition of “death.”
I haven't read the book, but the issue is described in a one-star review at Amazon:
The core of this linguistic mess is his inconsistent use of the word "death". At times he uses this term properly, as defined by the Uniform Determination of Death Act (UDDA, 1981): "An individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem is dead." This definition was developed in cooperation with the American Medical Association ... [etc.] and has been adopted by most states. It is the standard definition of death. [NOTE: I thought brain death is THE standard definition of death.] 1
Unfortunately, he also refers to "death" as cardiac arrest (e.g. pages 1, 2, 23, 42, 43, 128, 131, 139, 140, and many more). This definition of death is inconsistent with the UDDA because cardiac arrest is reversible in some cases. In fact, much of this book includes accounts of individuals who have suffered cardiac arrest and been resuscitated...
Dr. Parnia was quoted in my previous post about the “End of Life Gamma Waves” study in rats. He was skeptical that EEG during the 30 second interval after the heart stopped beating was anything more than a massive influx of calcium into the dying neurons. It wasn't a state of heightened consciousness that can explain the NDEs reported by 10-20% of his cardiac arrest patients.
Instead, Parnia is a mind-body dualist, believing that the soul (or self) can persist separately from the body for several hours at a time:
"It seems that when consciousness shuts down in death, psyche, or soul – by which I don't mean ghosts, I mean your individual self – persists for a least those hours before you are resuscitated. From which we might justifiably begin to conclude that the brain is acting as an intermediary to manifest your idea of soul or self but it may not be the source or originator of it… I think that the evidence is beginning to suggest that we should keep open our minds to the possibility that memory, while obviously a scientific entity of some kind – I'm not saying it is magic or anything like that – is not neuronal."
Memory is not neuronal! And Death can be cured. Who knew. But how?? [NOTE: according to Parnia and The Observer, at least.]
Extracorporeal membrane oxygenation (ECMO) is a temporary method of life support that introduces and circulates oxygen into the bloodstream of patients with acute respiratory failure or cardiac failure. It involves placing one or more large catheters into the patient's vessels (cannulation) and relies on an external pump to circulate and oxygenate blood and remove carbon dioxide (PDF). Primarily used in critically ill infants, its application to adults is risky and controversial, and the benefits are unclear.
A meta-analysis of ECMO in adult patients found a mortality rate of 54% at 30 day follow-up, with almost half the fatalities occurring during ECMO (Zangrillo et al., 2013). On the other hand, the procedure is a last-ditch life saving effort in critically ill patients, so a 46% survival rate seems like an improvement over probable death. However, one review stated that "Credible evidence for mortality benefit of ECMO is lacking" in cases of acute respiratory distress (Hirshberg et al, 2013). Another study concluded that ECMO is even less successful in cases of acute heart failure, with the worst survival rate for those who experience cardiac arrest (Tsuneyoshi & Rao, 2012).
Complications can be severe (Zangrillo et al., 2013) and include renal failure (occurring in 52%), bacterial pneumonia (33%), bleeding (33%), oxygenator dysfunction requiring replacement (29%), sepsis (26%), and liver dysfunction (16%).
The rest of the post will focus on the possible neurological complications of ECMO (Mateen et al., 2011).
Neurological Injury Associated with Heroic Resuscitation
I do not want to detract in any way from the dedication of practioners who do heroic things every day to save people's lives, or from advances in medicine. What I would like to point out, however, is that sometimes one may resuscitate the heart but lose the brain (to paraphrase Horstman et al., 2010).
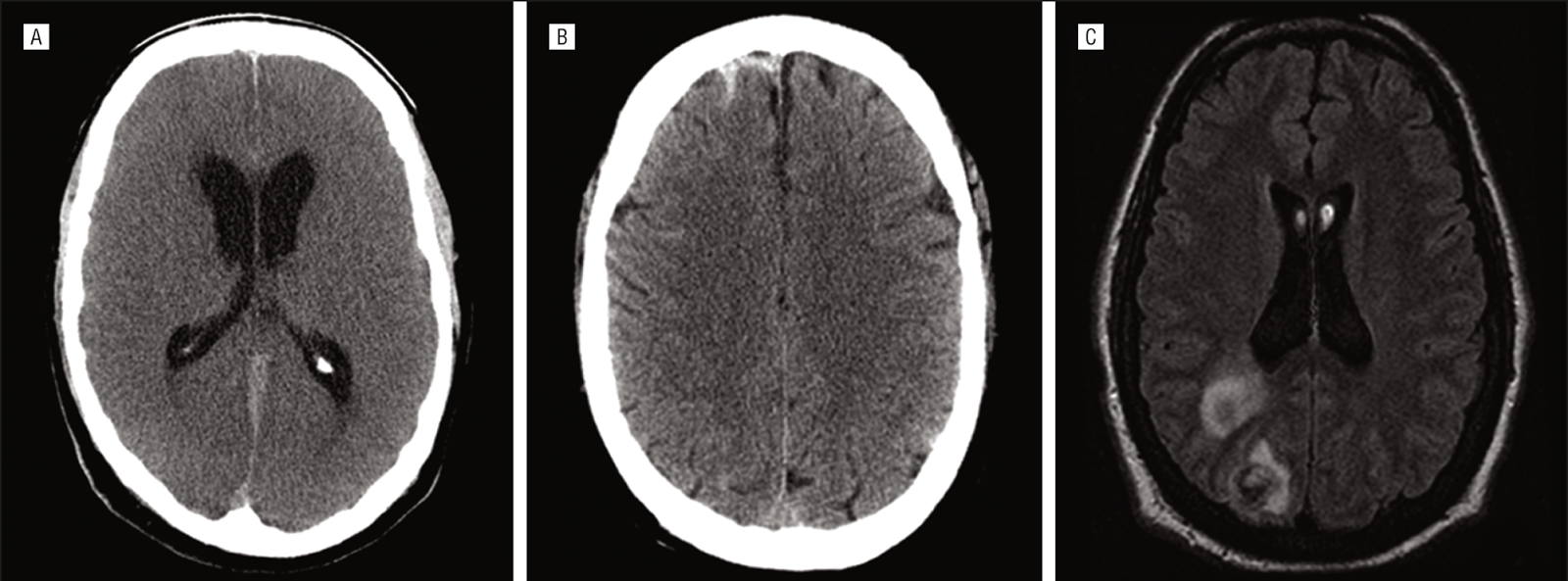
Neurological events occurred in at least 50% (n=42) of patients treated with ECMO at one medical center over an 8 year period (Mateen et al., 2011). This is a conservative estimate, because a neurological exam was not performed in 21%, and over 70% did not have neuroimaging. Clinical presentation included new onset of coma and new loss of brainstem reflexes. Diffuse brain injury due to lack of oxygen (anoxia), global brain dysfuction (encephalopathy), subarachnoid hemorrhage (bleeds), and ischemic watershed infarction (stroke) were among the diagnoses. Of the 24 patients with brain scans, the findings were pathologically abnormal in 15 (see examples in figure above).
Autopsy was performed on 10 brains (out of 40 patients who died). Nine of these brains showed gross abnormalities (see examples in figure below).

Brain sections stained for microscopic examination showed abnormalities in areas vulnerability to anoxia, including hippocampal pyramidal cells (the CA1 field) and cerebellar Purkinje cells. The hippocampus is a structure located in the medial temporal lobes that is critical for memory. Even mild hypoxia due to cardiac arrest (30 sec to 7 min until initiation of CPR) can lead to memory impairments. The residual cognitive deficits seen in post-cardiac arrest patients comatose for >24 hours have been well-characterized (Lim et al., 2004).
A group of 12 cardiac arrest survivors (not treated with ECMO) underwent MRI scans and neuropsychological testing (Horstman et al., 2010). Compared to controls, abnormalities in gray matter density were observed in regions important for memory and "drive" (subjectively rated motivation). ECMO is of course meant to preserve functioning of the brain and cardiopulmonary system, but I don't see how that's possible if the patient is "dead" for several hours.
Disclaimer: I am not a medical professional, and this post is not to be taken as medical advice.
Footnote
1 Actually, the definition of brain death is not entirely straightforward, either (Bacigalupo et al., 2007; Laureys, 2005).
References
Hirshberg E, Miller RR 3rd, Morris AH. (2013). Extracorporeal membrane oxygenation in adults with acute respiratory distress syndrome. Curr Opin Crit Care 19:38-43.
Horstmann A, Frisch S, Jentzsch RT, Müller K, Villringer A, & Schroeter ML (2010). Resuscitating the heart but losing the brain: brain atrophy in the aftermath of cardiac arrest. Neurology, 74 (4), 306-12 PMID: 20101036
Lim C, Alexander MP, LaFleche G, Schnyer DM, Verfaellie M. (2004). The neurological and cognitive sequelae of cardiac arrest. Neurology 63:1774-8.
Mateen FJ, Muralidharan R, Shinohara RT, Parisi JE, Schears GJ, & Wijdicks EF (2011). Neurological injury in adults treated with extracorporeal membrane oxygenation. Archives of Neurology, 68 (12), 1543-9. PMID: 21825216
Tsuneyoshi H, Rao V. (2012). The role of extracorporeal membrane oxygenation (ECMO) therapy in acute heart failure. Int Anesthesiol Clin. 50:114-22.
Zangrillo A, Landoni G, Biondi-Zoccai G, Greco M, Greco T, Frati G, Patroniti N, Antonelli M, Pesenti A, Pappalardo F. (2013). A meta-analysis of complications and mortality of extracorporeal membrane oxygenation. Crit Care Resusc. 15:172-8.

photo: Tanya Kozak












