
The 2012 Cognitive Neuroscience Society Meeting was held in Chicago from March 31 to April 3. The schedule was packed with three and a half days of symposia, slide sessions, and posters. One well-attended event was Symposium Session 2, on non-invasive brain stimulation.
Using Non-Invasive Brain Stimulation to Enhance Cognitive and Motor Abilities in the Typical, Atypical, and Aging Brain Chair: Roi Cohen Kadosh, University of Oxford
Speakers: Roi Cohen Kadosh, Jenny Crinion, Paulo S. Boggio, Leonardo G. Cohen
The talk by Dr Jenny Crinion, a speech and language therapist who has gone over to the "dark side" of research (as she put it), drew a lot of attention and media coverage. It's no wonder, given her clinically relevant results.
Jolt to brain aids language recovery Stroke patients improve on picture-naming task after stimulation treatment By Laura Sanders
Web edition : Monday, April 2nd, 2012 CHICAGO — A brain zapping technique helps people recover language after a stroke, new research shows. The results may point to a better way for people to relearn how to talk after a brain injury.
The "brain zapping" technique is transcranial direct current stimulation. According to a 2010 review by George and Aston-Jones, it is a very old method undergoing a recent revival:
Transcranial direct current stimulation (tDCS) is perhaps one of the simplest ways of focally stimulating the brain. Similar techniques were practiced almost immediately after electricity was 'discovered' in the late 1880s. Passing a direct current through muscle, or the brain, was in vogue in Europe. For example, one of Charcot's residents, Georges Duchenne de Boulogne, traveled around Paris with a small battery and passed electricity through patients' muscles, examining the effects on numerous disorders and using it to better understand muscle–nerve innervations, particularly in the muscular dystrophies (George, 1994).How does it work?
Quite simply, tDCS involves passing a weak (usually ≤ 1 mA) direct current through the brain between two electrodes. The current enters the brain from the anode, travels through the tissue, and exits out the cathode. Some researchers refer to this as either cathodal tDCS or anodal tDCS depending on which electrode is placed over the region that is being modified (Figure 5).
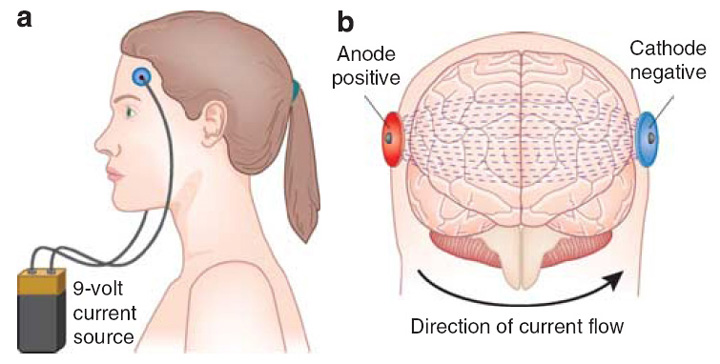 Figure 5 (George & Aston-Jones, 2010). A tDCS device uses an anode and cathode connected to a direct current source much like a 9 V battery (a). The direct current passes through the intervening tissue, with some shunting through the skull but much of it passes through the brain and changes resting electrical charge, particularly under the cathode (b).
Figure 5 (George & Aston-Jones, 2010). A tDCS device uses an anode and cathode connected to a direct current source much like a 9 V battery (a). The direct current passes through the intervening tissue, with some shunting through the skull but much of it passes through the brain and changes resting electrical charge, particularly under the cathode (b).Crinion started her talk by saying she originally wanted to use transcranial magnetic stimulation (TMS) -- another non-invasive brain stimulation technique -- but this would be too painful if applied over the left inferior frontal cortex (Broca's area). She lamented the NHS limit of 12 hours of speech therapy for stroke patients with aphasia. These individuals would benefit from more intensive therapy (e.g., phonemic cueing) for a longer period of time. From a practical standpoint, then, would tDCS maximize the results obtained during a truncated retraining period?1 What sort of behavioral and neural effects might be expected with such a regimen?
She continued by describing a study in control participants that combined behavioral priming for overt picture naming, true and sham tDCS, and fMRI (Holland et al., 2011). Anodal tDCS2 was applied over the left IFC.3
What are the effects of tDCS on echo planar imaging (EPI)? Any potential for artifacts, you ask? No problem! Supposedly there's signal dropout at the scalp/skull but not the brain. See?

This is what I first saw on the slide. "EPI is not affected," apparently, but the images looked mighty odd to me. What the &^$% kind of brain is that??
It's not a brain, it's a watermelon! Oh...
Figure S1. Effects of A-tDCS on Echo-Planar Images (EPI). Field distortions from control (watermelon) and one participant.
(A) Multi-slice coronal view of watermelon field distortion with indices for each slice. Blue bar indicates the location of anodal electrode... Perturbations were localized to the surface layer only of the watermelon.
Here's more, from Holland et al. (2011).
 Figure S1. (D) Consistent with the control data, perturbations in the participants’ data were also localized to the scalp surface only. Here we illustrate in one participant’s coronal sections the effect of the anode electrode on B0 field map data.
Figure S1. (D) Consistent with the control data, perturbations in the participants’ data were also localized to the scalp surface only. Here we illustrate in one participant’s coronal sections the effect of the anode electrode on B0 field map data.All right, so what were the effects of tDCS on picture naming times?

My god, what a giant effect! Oh wait... It's more like a 25 msec improvement (see below), which is still statistically significant.4

Figure 1 (modified from Holland et al., 2011). Behavioral Effects of Anodal Transcranial Direct Current Stimulation. Main effects of order, i.e., position of run during scanning session (P1 versus P2; A) ... and stimulation (sham vs. A-tDCS; C), on naming reaction times (n = 10). ... Error bars indicate standard error of the mean (SEM). ∗∗∗p < 0.001, ∗∗p < 0.05.
How about the effects of tDCS on the BOLD response? Briefly, stimulation decreased naming-related activity in two localized regions: left inferior frontal sulcus and left ventral premotor cortex (suggestive of neural facilitation):
A-tDCS—by depolarizing neurons nearer to threshold—can reduce the amount of excitatory input required to produce a naming response. Thus, we can have a situation in which there is increased excitability (manifest as a faster response time to a given input) accompanied by reduced BOLD (less synaptic input for a given output, in this case naming).Finally, the preliminary results of a clinical study were presented. Thirteen participants with aphasia received 60 hours of behavioral training with specific pictures. Patients receiving tDCS over intact left IFC (n=6) or sham stimulation (n=7) were compared. Picture naming accuracy for the trained items improved by 56% in the sham group and by 92% in those getting real stimulation. There was no improvement on the untrained items in either group.
These results are very impressive. However, a quick PubMed search of tDCS, aphasia revealed 20 published articles already5 [which was surprising to me, as it wasn't mentioned in the talk. Or else I forgot about it. Or didn't hear it]. Turns out some of these were reviewed in Holland and Crinion (2011). Nevertheless, none of this detracts from the current findings:
This gap persisted after the initial testing, though it diminished in size. Three months out, volunteers who received the stimulation performed 82 percent better than they had performed before treatment, while those receiving sham treatment held steady with a 55 percent improvement. “These are huge effects,” Crinion said. “It’s really encouraging.”The 3 month followup is longer than previous studies (e.g., Baker et al., 2010; Fridriksson et al, 2011; Marangolo et al., 2011). Crinion and colleagues also plan on publishing the brain imaging results from their ongoing trial.
Where do things go from here? DIY treatment kits? Perhaps (Holland & Crinion, 2011)...
Due to its appeal as a potential treatment tool, some manufacturers (NeuroConn, Germany, personal communication) are exploring mini-tDCS kits for patient's self-administration at home with stimulation dosages pre-programmed by their clinician. Some additional precautions should be considered for safe use of tDCS: (i) patients should have no metallic implants near the electrodes, and (ii) personnel conducting tDCS should be appropriately trained before applying the technique, as experience with the method is still limited and the risk profile of stimulation is not yet completely known.

Further Reading:
Give your brain an electric shock, learn stuff fasterHow To Electrify Your Brain To Be Smarter With a 9-Volt Battery -- Kids! Don't try this at home!DARPA Study Uses Video Game to Research tDCS, Finds More Amps Mean More FragsAustralian Researchers Create “Thinking Cap”, Scheme to Breed Army of Nobel Laureates and Mad ScientistsNeurostimulation - The Genius Machine? -- covers the latest from Richard Chi and Allan "thinking cap" Snyder.
Footnotes
1 Surprisingly, the NHS website mentions both tDCS and TMS as treatment modalities for aphasia, although no coverage is provided.
It has been suggested that both tDCS and TMS may help to stimulate parts of the language centre that have been damaged and encourage a certain degree of recovery and repair. For example, initial research has found that these types of treatment may help people to improve their ability to remember the names of certain objects, people and places. As transcranial stimulation is a new method of treatment, access is currently limited to people who are willing to take part in a clinical trial.2 Anodal tDCS (A-tDCS) is thought to increase cortical excitability.
3 MNI coordinates were -48 20 19. More about location and parameters:
A-tDCS stimulation was generated by a specially designed MRI-compatible neuroConn stimulator system and delivered at 2 mA continuously for 20 min via a pair of identical MRI-compatible leads and rectangular rubber MRI-compatible electrodes (5 × 7 cm), allowing for a current density of 0.057 mA/cm2. For all participants, the anode was placed over the left IFC (equivalent to electrode position FC5 in a 10-10 EEG nomenclature), with the cathode placed over the contralateral frontopolar cortex.4 More fine print...
Participants were selected based on previous behavioral performance during a speech-priming fMRI task. The main criterion for selection was a word versus control cue priming effect of greater than 85 ms....and:
Participants reported no adverse sensations during A-tDCS and sham. They could detect a difference between the two conditions (p = 0.07), but they were unable to reliably distinguish which was A-tDCS.5 Not all of these were double-blind treatment studies, though.
References
Baker JM, Rorden C, Fridriksson J. (2010). Using transcranial direct-current stimulation to treat stroke patients with aphasia. Stroke 41:1229-36.
Fridriksson J, Richardson JD, Baker JM, Rorden C. (2011). Transcranial direct current stimulation improves naming reaction time in fluent aphasia: a double-blind, sham-controlled study. Stroke 42:819-21.
George, M., & Aston-Jones, G. (2009). Noninvasive techniques for probing neurocircuitry and treating illness: vagus nerve stimulation (VNS), transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS). Neuropsychopharmacology, 35 (1), 301-316. DOI: 10.1038/npp.2009.87
Holland, R., & Crinion, J. (2011). Can tDCS enhance treatment of aphasia after stroke? Aphasiology, 1-23. DOI: 10.1080/02687038.2011.616925
Holland, R., Leff, A., Josephs, O., Galea, J., Desikan, M., Price, C., Rothwell, J., & Crinion, J. (2011). Speech Facilitation by Left Inferior Frontal Cortex Stimulation. Current Biology, 21 (16), 1403-1407. DOI: 10.1016/j.cub.2011.07.021
Marangolo P, Marinelli CV, Bonifazi S, Fiori V, Ceravolo MG, Provinciali L, Tomaiuolo F. (2011). Electrical stimulation over the left inferior frontal gyrus (IFG) determines long-term effects in the recovery of speech apraxia in three chronic aphasics. Behav Brain Res. 225:498-504.
No comments:
Post a Comment